- This topic is empty.
-
AuthorPosts
-
-
May 8, 2025 at 3:14 am #9790
Farrydesigner
KeymasterA new Bureau of Justice Statistics report offers updated data on pregnancy among people in state and federal prisons. This important new dataset includes the prevalence of pregnancy among incarcerated people, pregnancy outcomes, and some limited data on the types of services, medical care, and support offered to incarcerated pregnant people. The findings from Maternal Healthcare and Pregnancy Prevalence and Outcomes in Prisons, 2023 are based on data collected for the first time in 2024 as a supplement to the annual National Prisoner Statistics survey. While this report is a welcome contribution to a shamefully understudied experience during incarceration, the data it provides raises almost as many questions as it answers.
Women’s incarceration has grown at twice the pace of men’s incarceration in recent decades but there is often too little data to explain this growth or to elaborate the specific effects incarceration has on women and their health, including their experience of pregnancy.1 Previously, the most recent national data on pregnancy in prisons from the Bureau of Justice Statistics was collected in the Survey of Prison Inmates in 2016 and was published in 2021. Since then, researchers from Johns Hopkins University collected detailed data on pregnancy outcomes in a smaller set of 22 state prison systems and the federal Bureau of Prisons from 2016 to 2017 as part of the Pregnancy in Prison Statistics (PIPS) study. Even though the PIPS study covered only about half of state prison systems surveyed by the Bureau of Justice Statistics, the findings offered a closer look at pregnancy outcomes in prison than were available from the Survey of Prison Inmates. In this new publication, the Bureau of Justice Statistics surveyed 50 state departments of corrections and the federal Bureau of Prisons regarding:
- the number of pregnancy tests provided and found positive upon admission to prison,
- the number of pregnant people in prison at year-end,
- the outcomes of the more than 700 pregnancies that ended in prison in 2023, and
- the availability of specific kinds of pre- and post-natal support across jurisdictions.
Yet the data raises a series of new questions. There are unexplained differences in the prevalence of pregnancy behind bars compared to the PIPS report, as well as a lack of basic data on the outcomes of live births, and a failure to report how often pregnancy-related services and accommodations are actually used. The report also helpfully touches on services like prison nursery programs; however, crucial details about their implementation are left out — a gap we attempt to fill in this briefing using our own research. This new report is a step in the right direction, but much more work needs to be done to provide an accurate and useful portrait of pregnancy in prison.
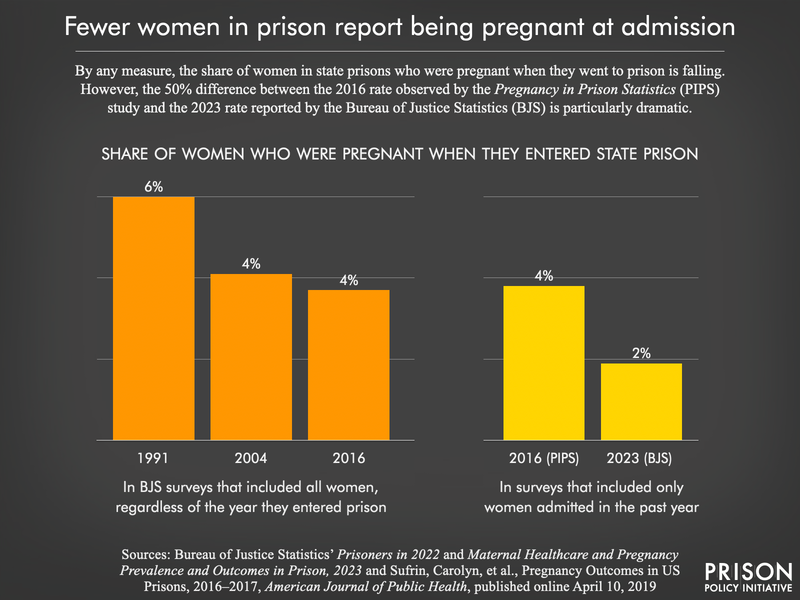
Fewer people in prison report being pregnant when entering prison
The prevalence of pregnancy in prisons is measured in two ways: the number of pregnant people admitted to prison over the course of the year and the number of pregnant people in prison on a single day. The Bureau of Justice Statistics reports that 2% of women tested upon admission were pregnant in 2023.2 This is surprisingly low compared to findings from previous data collection. In 2016, twice as many women (4%) admitted to prison each month were pregnant, according to the Pregnancy in Prison Statistics (PIPS) study. Past surveys from the Bureau of Justice Statistics that asked incarcerated women whether they were pregnant at admission (regardless of what year they were admitted) also found higher rates, from 6% in 1991 to about 4% in 2016. While the PIPS project surveyed only 22 state prison systems, it seems unlikely that this difference in the sample would explain the inconsistency in the data.3
We see this same issue in the point-in-time count of incarcerated pregnant people. According to the Bureau of Justice Statistics, on a single day in 2023 , there were 328 pregnant people in state (0.5%) and federal (0.3%) prisons, representing a total of 0.5% of all women in prison. This is much lower than we would expect based on the 2016 Pregnancy in Prison Statistics (PIPS) data, which found there were 350 pregnant people in just the smaller group of state (0.7%) and federal (0.3%) prisons they surveyed, for a total of 0.6% of the combined prison population. In other words, the actual number of pregnant incarcerated people was higher in the PIPS report that covered half as many state prison systems (22 states) as the Bureau of Justice Statistics report. It’s unclear what accounts for this substantial difference in the datasets.
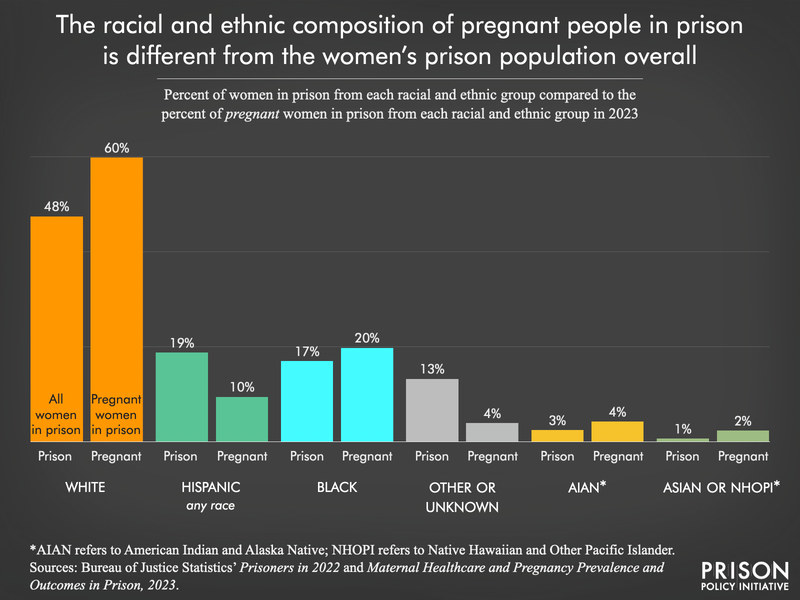
The new Bureau of Justice Statistics report also offers new data on the race and ethnicity of pregnant people in prison on a single day. Compared to the overall population of women in prison,4 white, Black, American Indian and Alaska Native, and Asian women are overrepresented in the population of pregnant people in 2023. Meanwhile, Hispanic and “other” women were underrepresented.
Certainly, some decline in the number of pregnant people in prison could be expected, given that the national pregnancy rate in the United States has been steadily falling over the past two decades.5 However, this trend does not explain the dramatic reduction in the number of pregnant women in prison between the PIPS 2016 study and the Bureau of Justice Statistics’ 2023 report. Given the limited data available, we do not have any clear understanding of why there are so many fewer pregnant people reported in this Bureau of Justice Statistics publication.
First national data on pregnancy outcomes in prisons
This Bureau of Justice Statistics report is significant in that it offers the first national data on pregnancy outcomes in prisons — a welcome if overdue development. More than 700 pregnancies ended while the mother was in custody in 2023, and almost all of these were live births (91.5%),6 with 6.5% ending in miscarriage and 2.1% ending in abortion.7 Additionally, there were four stillbirths and ectopic pregnancies. These percentages are largely consistent with the outcomes of pregnancies reported in the Pregnancy in Prison Statistics (PIPS) study from 2016, however the counts are once again surprisingly low: in 2016, PIPS found 816 pregnancies ended in 22 state prison systems and the federal Bureau of Prisons, but in 2023, the Bureau of Justice Statistics reported 89 fewer pregnancies ending in prison (727 total) across the federal system and 48 state departments of correction.
Nationally, data on pregnancy outcomes regularly includes information about the outcomes of live births, including if they were preterm, early term, C-sections, or low birthweight, as well as if there was neonatal death (within 28 days) or maternal death following the birth. Although the U.S. Centers for Disease Control and Prevention regularly collects and publishes these data for non-incarcerated people, the Bureau of Justice Statistics survey did not request this information from correctional authorities, despite our recommendation during the public comment period. Basic national statistics on pregnancy in prison can and should include these outcomes. Elevated rates of chronic and infectious diseases – as well as substance use disorders – and limited access to necessary healthcare among incarcerated people make more detailed data about live births critical to understanding the experience of pregnancy in prison. Such data can also inform the interventions and medical treatments required to promote health before, during, and after birth for this population.
Some prisons fail to provide even the most basic prenatal and postnatal care
Pregnancy poses a number of short-term and long-term risks to health. Globally, the United States has one of the highest rates of pregnancy-related complications among developed nations,8 with a disproportionate burden falling upon women of color and low-income women.9 Addressing such risks is particularly important in prisons, where women already face higher rates of chronic health conditions, substance use disorders, and mental health conditions, as well as a history of poor healthcare access. Decarceration is the most important tool we have to address these risks, however as long as our society incarcerates pregnant people, prisons must be prepared and equipped to provide them with adequate healthcare and support before, during, and after delivery.
Most prison systems reported they train staff to care for pregnant people (88%) and have an onsite infirmary (96%) or 24/7 or on-call medical care (98%). The majority of prison systems also reported that they provide medical appointments to pregnant people within two weeks of a positive test (96%), routinely throughout the pregnancy (100%), and within three weeks of delivery (96%). Prison systems claimed that these services are available, however there is no information in the report about their actual utilization. Does every pregnant person have an appointment within two weeks of a positive pregnancy test and within three weeks of delivery? Do all staff receive training regarding pregnancy, or only healthcare staff? These questions are arguably more important than whether these services and practices technically exist.
It is particularly troubling that six state prison systems (Alaska, Hawaii, Iowa, Maine, Nevada, and Washington) reported that they do not provide any staff training regarding pregnant people in prison. No state prison system is immune from admitting a pregnant person, and these six states accounted for around 5% of the almost 50,000 women admitted to prison in 2021.10 At the very least, corrections and healthcare staff should receive training regarding emergency responses that may be required with a pregnancy.
Postpartum depression is another serious risk facing pregnant people. Nationally, postpartum depression diagnosis rates have been climbing: across all racial and ethnic groups, the rate of diagnosis increased from 9% in 2010 to 19% in 2021. Undoubtedly, this trend persists behind bars, where women face a number of risk-factors for postpartum depression. This includes previous mental illness diagnosis,11 a lack of social support, poor prenatal and perinatal healthcare, separation from the newborn, and experiencing partner violence. In one study of 58 people who gave birth while in prison, researchers found that more than one-third of participants met the diagnostic criteria for moderate to severe depression during pregnancy or postpartum. Yet four state prison systems (Alabama, Iowa, Massachusetts, and Washington) said they do not provide depression screenings during pregnancy or postpartum. Not screening for depression at all during pregnancy and the postpartum period is a failure to meet the most basic standards of pregnancy-related care.
The Bureau of Justice Statistics report also provides information about which state prison systems provide certain accommodations and support services to people before and after delivery. Prison systems universally reported furnishing at least two accommodations for pregnant people: lower bunk placement12 and prenatal vitamins.13 Most (but not all) prison systems offer a special diet during pregnancy (86%) and consultation with social workers (92%) or psychologists (88%). Prenatal diets require increased calories and a particular balance of nutrients that are likely not met by the typical prison diet. Accessible, appropriate mental health services for pregnant people behind bars are also vitally important, and most standards for pregnancy-related health care in correctional settings emphasize the need for counseling and psychosocial support.
Other extremely basic accommodations are less common in prison systems. These include a special postpartum diet (60%), doula support (35%),14 extra pillows during pregnancy (69%), and breast pumps (78%). These relatively simple interventions can have a tremendous impact during pregnancy and postpartum. For instance, the recommended postpartum diet is associated with fewer symptoms of postpartum depression and can positively impact infant health. People in prison are regularly issued only one pillow, but pregnant people may require more to be comfortable and avoid sleep deprivation, which has been associated with longer labor, elevated perception of pain and discomfort during labor, higher cesarean rates, preterm labor, and other adverse outcomes. While policies may be in place for breast pumping accommodations in most prison systems, the actual accessibility and utilization of breast pumps may be a different story. Some prison systems operate lactation programs that allow incarcerated people to pump breast milk for their babies. However, these programs often have onerous requirements for the incarcerated person’s friends and family, who have to apply for approval to visit and collect the milk. In Florida, for example, incarcerated people are only eligible for this program if there is an approved guardian for the child and the child is not placed in state custody. Reports suggest that when there is no lactation or pumping program, incarcerated people are sometimes not allowed to breastfeed after giving birth,15 and are not provided with anything to help manage an unused milk supply or information about what to expect.
It’s undoubtedly helpful to know which jurisdictions offer these services, but there is once again no information regarding their actual utilization. In 2016, self-reported data from incarcerated people revealed that half of people pregnant upon admission had not received prenatal care in the form of special testing, dietary changes, or childcare instruction. It’s great that prison systems have policies in place to provide these necessary services, but it is not clear at all how they are being implemented and how many pregnant people actually receive them.
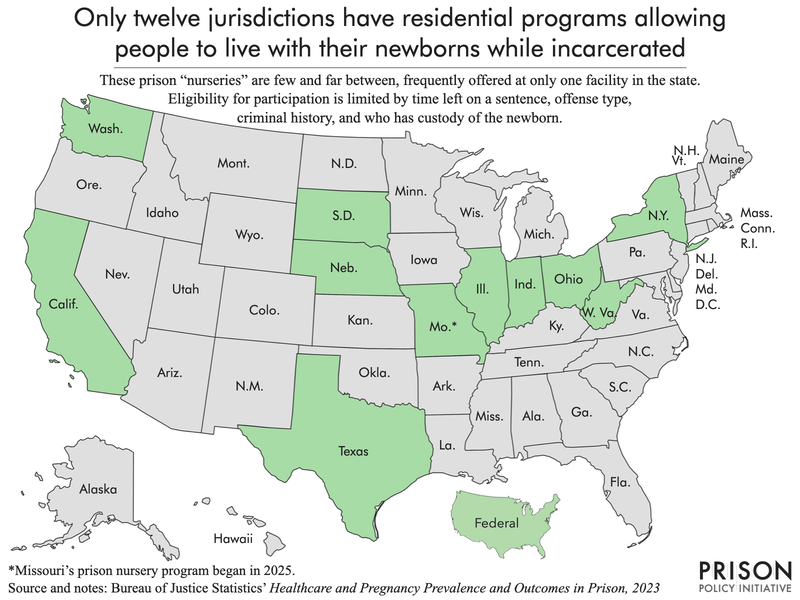
Only 11 states and the federal system operate prison nursery programs where newborns can reside with their parents in custody
The Bureau of Justice Statistics reported that ten states and the federal Bureau of Prisons run prison nursery programs, which are residential programs where people can live with their newborns. Although reducing the incarceration of pregnant people is the best approach to this issue, prison nurseries can be another option that allows incarcerated mothers to avoid separation, and to be with and care for their newborn children. Since the data collection period ended for this report, an eleventh state — Missouri — opened their prison nursery program. Even though there were 665 live births in prisons across the U.S. in 2023, only 86 people were participating in prison nursery programs at the end of the year. In Nebraska and West Virginia, there were no nursery program participants at the end of the year.
There are a number of details about these prison nursery programs lacking in the Bureau of Justice Statistics report. For example, how many people participate in the programs each year and for how long? What programming is available to the participants while in the nursery program? How is eligibility determined for participating in these programs? Again, while data on the number of nurseries is helpful, it’s arguably more important to know how they are being used. So, to better understand how prison nursery programs actually work, we looked at the eligibility requirements and restrictions for prison nursery programs in 11 states and the federal Bureau of Prisons.
We found that in all but one of the prison nursery programs, participation requires release dates within 12 to 36 months of the expected delivery date.16 A number of factors can influence eligibility, including offense types, prison disciplinary history, medical or mental health status, prior Child Protective Services involvement, and prison security designation or classification. In Illinois, for example, any child that requires “more than normal well child health care” or any parent requiring “more than normal” prenatal or postnatal care can be excluded from the program. In California, Illinois, Indiana, Ohio, and West Virginia, the incarcerated mother must have sole legal custody of the child. To our knowledge, there are no data available about how often a child born to an incarcerated parent remains in their custody, but there is historical evidence to suggest that this is likely rare, or at the very least, complicated.
Eligibility requirements and considerations for prison nursery programs
For more details and sourcing, see the Appendix Table. Jurisdiction Pregnant on prison admission Disciplinary record Current or prior offense Medical or mental health Legal custody of newborn California ✓ ✓ ✓ ✓ Federal ✓ ✓ ✓ ✓ Illinois ✓ ✓ ✓ ✓ Indiana ✓ ✓ ✓ Missouri ✓ Nebraska ✓ ✓ ✓ New York Ohio ✓ ✓ ✓ South Dakota ✓ Texas ✓ Washington ✓ ✓ ✓ West Virginia ✓ ✓ ✓ Unfortunately, because the Bureau of Justice Statistics report does not include information on the sentence length, offense type, prior convictions, or classification status of pregnant people in prison, it is difficult to estimate how many pregnant people in prison would be eligible for these programs. These potentially beneficial programs are a vast improvement over the common practice of simply removing newborn children from their parent at birth.17 However, access to nurseries is still seriously limited, and ultimately, the best option would be to implement caregiver mitigation and diversion laws and prevent the incarceration of pregnant people.
Conclusion
This Bureau of Justice Statistics maternal healthcare report marks an important step toward filling the huge data gap regarding the incarceration of pregnant people in prisons. Given their particular healthcare needs and the challenges to a healthy pregnancy imposed by the prison environment, these data can help inform interventions that lead to better outcomes for incarcerated pregnant people. Although the data answer some of our initial questions about how many pregnant people enter prison and what jurisdictions have policies offering specific supports, significant questions remain. In addition to getting to the bottom of why the findings in the Pregnancy in Prison Statistics study differ so substantially from the Bureau of Justice Statistics survey, future researchers can make important contributions by answering questions such as:
- What are the trends in pregnancy in prison over time? Why are these estimates of the prevalence of pregnancy in prison lower than prior estimates?
- How many people actually receive the services that these jurisdictions report offering?
- What barriers do prison systems face in providing the most basic prenatal and postnatal care, like depression screenings?
- Why are so many pregnant people incarcerated (i.e, for what offenses) and for how long (i.e., sentence length)?
- What are the outcomes of the live births counted in this report (i.e., preterm, early term, C-sections, low birthweight)? What are the rates of neonatal death and maternal death among this population?
Data on maternal healthcare and pregnancy outcomes should continue to be collected and published on a regular basis by the Bureau of Justice Statistics. Doing so — especially in greater detail — would shed light on an important and understudied healthcare experience in prison.
Appendix table: Detailed eligibility requirements and considerations for participation in prison nursery programs
Jurisdiction Release eligibility date Pregnant on prison admission Classification Disciplinary record Current offense and sentence Prior convictions Medical or mental health Prior Child Protective Services involvement Legal custody of newborn Source California Wthin 6 years of birth18 Exclusion: found guilty of a serious rule violation Exclusion: sex offenses, violent offenses (some can be reviewed case-by-case), arson offenses, escape or aiding escape convictions, active detainer (unless for failure to appear or misdemeanor motor vehicle violations) Exclusion: previously removed from a community program resulting from violation of state laws, rules, or regulations in California Department of Corrections and Rehabilitation Exclusion: staff physician or psychiatrist assessment Exclusion: found “unfit parent in any court proceeding” Requirement: primary caretaker of the infant prior to incarceration (if born prior to incarceration) CA Penal Code S 3417 (2024) Federal19 Within 30 months of due date Requirement: must be pregnant when admitted Requirement: minimum security Exclusion: disciplinary violations of “an aggressive/assaultive nature” or for any “200 or higher series incident reports” in prior 6 months Exclusion: convictions for sex offenses, crimes against a child, domestic violence or other violent convictions Requirement: “be physically and mentally capable of caring for a child as determined by medical and mental health staff” Exclusion: current no-contact orders with minor children, contact-founded allegation or inconclusive referrals for neglect or abuse with Child Protective Services Female Offender Manual (2021) Illinois Within 24 months of delivery Consideration: grade, security designation, and escape risk Consideration: disciplinary history Consideration: outstanding warrants or detainers, the nature and class of the offense, sentence, including factors such as the nature and class of the offense, length of sentence, and sentencing orders consideration: history of violence, abuse, criminal neglect, sexual offenses, or crimes against children, affiliation with organized crime activities or narcotics trafficking Consideration: medical or dental health, psychological evaluation Consideration: Department of Children and Family Services involvement, including, but not limited to, present or past investigations or cases regarding the offender and her children, court order prohibiting contact with children Requirement: the baby “shall be in the custody of his or her mother” or “obtain consent from the father for the baby to participate in the Program” Illinois Department of Corrections press release (2010) & 20 IL Admin Code S 475.20 Indiana Within 26 months of due date Requirement: must be pregnant when admitted Consideration: charged with a sex crime or any type of violence, abuse or endangerment of a child Requirement: sole, legal custody Department of Corrections Leath MCU Eligibility Criteria Missouri Within 18 months of delivery Exclusion: dangerous felony, sexual offense, or offenses against the family convictions Missouri SB 834 (2022) Nebraska Within 24 months of delivery Requirement: must be pregnant when admitted Exclusion: a long list of offenses including manslaughter and murder, as well as robbery and arson.20 Consideration: pending charges Consideration: mental health history Exclusion: history of child abuse as determined by state Department of Health and Human Services and file history Received via email communication with the Nebraska Department of Correctional Services. New York Within 18 months of delivery21 NY Corr L S 611 (2024) Ohio Sentence of 36 months or less Requirement: must be pregnant when admitted Exclusion: violent crime or any type of child abuse, or child endangerment conviction Requirement: sole, legal custody OH Admin Code S 5120-9 (2023) South Dakota Within 30 months of delivery Exclusion: a long list of offenses including manslaughter, murder, rape, robbery, as well as arson, burglary, and violation of a drug-free zone.22 Consideration: pending charges, outstanding warrants. Exclusion: removal of a child by the state. Consideration: child abuse will be determined on crime, past history, inquiry to, and response received by Department of Social Services (DSS) Child Protection Services (CPS). Policy 300-25 (2024) Texas Within 12 months of due date Requirement: minimum custody Exclusion: past or current conviction for any violent offense, arson or “an offense that would require registration as a sex offender” Exclusion: past or current conviction for any violent offense, arson or an offense that would require registration as a sex offender Department of Criminal Justice press release (2015) Washington Within 30 months of birth Requirement: must be pregnant when admitted Requirement: minimum (MI)2 or MI1 custody level Exclusion: conviction for a crime against chidlren per RCW 28A.400.322, conviction for “a sex offense(s) and/or sexual motivation behavior” Requirement: vaccinations for annual influenza, MMR, Tdap Requirement: approved by Child Protective Services. Exclusion: current no contact order with minor children Policy 590.320 (2023) West Virginia Within 18 months of delivery Requirement: must be pregnant when admitted Requirement: internal classification of the division Requirement: “be physically and mentally capable of caring for a child” Requirement: assessed by Child Protective Services (CPS) and cleared of any history of abuse and/or neglect Requirement: sole, legal custody Reporting from States of Incarceration & WV Code S 25-1B (2024) Footnotes
-
We acknowledge that people of many different gender identities can become pregnant. Unfortunately, the data published by the Bureau of Justice Statistics is not broken down by gender identity. Instead, it relies on administrative data, which is primarily reliant on the binary sex variables of male and female. The report presents data exclusively about women in the custody of state and federal correctional authorities and female admissions, ostensibly conflating “women” with administratively-identified “female” people. ↩
-
Not all women admitted to prison were given a pregnancy test: more than 7,500 women admitted to state prisons (13%) and about 470 women admitted to federal prisons (7%) were not tested. ↩
-
In fact, the 22 states included in the Pregnancy in Prison Statistics (PIPS) study had a lower average pregnancy rate (85.7 per 1,000 women aged 15-44) in 2016 than the total U.S. (89.6 per 1,000). We would therefore expect a higher reported pregnancy rate in the Bureau of Justice Statistics study that included states with higher pregnancy rates overall. ↩
-
At the time of this publication, the Bureau of Justice Statistics has not yet published race and ethnicity data for the 2023 prison population. For this comparison, we rely on the race and ethnicity of the sentenced prison population on December 31st, 2022, published in Table 10 of Prisoners in 2022. ↩
-
The pregnancy rate in the United States — calculated from the number of live births, pregnancy losses, and abortions — has been steadily declining since 2010. In 2016, the pregnancy rate was 89.6 per 1,000 women aged 15-44, and in 2020, this rate decreased by 8% to 83 per 1,000. ↩
-
Pregnancies resulting in live births were more common (91.5%) in prison in 2023 than in the total national population in 2020 (67%). ↩
-
Notably, abortions are more common outside prison (17% of pregnancies in 2020) than in prison (2% in 2023). Research shows that even in states where abortion is legal, many incarcerated people may be effectively blocked from obtaining the care they need, thanks to insurmountable barriers like self-payment requirements and physical distance from abortion caregivers. ↩
-
In 2023, the maternal mortality rate (calculated as the number of maternal deaths per 100,000 live births) in the United States was 17 per 100,000, more than double that of the United Kingdom (8 per 100,000) and higher than most other comparable developed nations. ↩
-
While maternal mortality rates are unacceptably high in the United States across the board, Black and American Indian and Alaska Native women are at increased risk for pregnancy-related death. Black women are three times more likely to die from pregnancy-related complications than white women. Women with lower socioeconomic status are more likely to face a number of serious pregnancy outcomes than those with the highest household incomes. ↩
-
In 2021, there were 49,038 women admitted to state and federal prison and 2,269 were admitted to those six states’ prison systems (Bureau of Justice Statistics, CSAT-Prisoners). More recent admissions data broken down by sex have not yet been published. ↩
-
Two thirds of women diagnosed with postpartum depression had depression prior to or during pregnancy. Other mental health conditions (prior to childbirth) including anxiety, PTSD, and bipolar disorder are also associated with postpartum depression. Rates of mental health conditions are extremely high among imprisoned women: 69% of women in state prison and 52% of women in federal prison have a history of a mental health problem, with 19% of women in state prisons and 17% in federal prisons reporting serious psychological distress in the past 30 days. ↩
-
Climbing onto a higher bunk is a risk factor for falling. Falls during pregnancy can result in fractures and sprains for the pregnant person, as well elevated risk for preterm labor, placental abruption (separation from the uterus), fetal distress, and fetal hypoxia. ↩
-
Prenatal vitamins are part of the basic standard of care for pregnant people: the use of prenatal vitamins can prevent 50-70% of neural tube defects, as well as other negative outcomes. ↩
-
Doulas are professionals who provide continuous support and comfort during pregnancy, delivery, and the postpartum period. Their presence is associated with positive delivery outcomes, including fewer cesarean sections and premature deliveries, as well as shorter labors. Doula support is also associated with reduced anxiety and stress and improved breastfeeding success. ↩
-
There are a number of potential serious complications associated with early weaning, including increased risks of breast cancer, ovarian cancer, diabetes, hypertension, and heart attacks. While people may choose not to breastfeed, the forced early weaning that inevitably occurs in prison is in-and-of-itself risky. ↩
-
The exception is California: “a probable release or parole date with a maximum time to be served of six years, calculated after deduction of any possible good time credit.” ↩
-
While we do not know the custody status of newborns born to incarcerated people, we do know that ultimately, incarcerated mothers are five times as likely to have their children placed in foster care and are more likely to have their parental rights terminated due to incarceration than fathers. ↩
-
People who were the primary caretaker of a child under six years of age prior to incarceration can also apply to the California Prisoner-Mother Program (CPMP). ↩
-
This is “an inter-governmental agreement with the Washington Department of Corrections (WADOC) to place qualified, interested pregnant inmates in the RPP at the Washington Correctional Center for Females in Gig Harbor.” ↩
-
The full list of current or past offenses that result in exclusion from the program is as follows: “1st and 2nd degree murder, manslaughter, 1st degree sexual assault, 1st degree assault, robbery, all other sexual assault offenses, stalking involving a minor, kidnapping/false imprisonment involving a minor, arson, child abuse (as determined by DHHS and file history), incest, other serious crimes against children, any other serious offenses that could place the child in jeopardy” (including attempts, conspiracy or solicitation to commit these offenses). ↩
-
People who are nursing a child under on year old at time of prison admission can also apply to the program. ↩
-
The full list of current or past offenses that result in exclusion from the program is as follows: “manslaughter 1st and 2nd, murder 1st and 2nd, rape all, robbery (all), arson (all), burglary 1st, commission of a felony while armed with firearm (all), possession of a weapon by offender, criminal pedophilia, possession of weapon in jail, aggravated assault – baby (includes subsequent offense), aggravated assault against law enforcement, child abuse (all), sexual contact (all), vehicular homicide, vehicular battery, removal of a child from state, stalking (includes 1st felony offense, subsequent offense and child 12 or younger), discharging a firearm at an occupied structure or motor vehicle (with bodily injury), photographing child in obscene act, possession of a firearm by a felon, sliming (felony), indecent exposure (all), simple assault (all), possession of child pornography, incest (all), discharging a firearm from a moving vehicle, sexual exploitation of a child (includes subsequent offense), threatening to commit a sexual offense, solicitation of a minor (includes subsequent offense), riot (all), enticing away a child, violation of drug free zone (reviewed on a case-by-case basis), distribution of drugs/controlled substance/flunitrazepam to a minor, permitted physical or sexual abuse of a child” (including attempts, conspiracy, solicitation to commit, or accessory to these offenses). ↩
-
-
AuthorPosts










- You must be logged in to reply to this topic.